Thanks Jennifer for the reference to Physiology of Bone Formation, Remodeling, and Metabolism by Usha Kini and B. N. Nandeesh. I read through it and took some notes, and then followed up with some other readings. My notes are are a bit long-winded as they are mostly quotes. For those who don't want to wade through them, I have put them at the end.
It seems to me that while 'bone growth' per se may cease at puberty as you have suggested, 'bone remodelling' can continue for all your life. What's more, this 'remodelling' can add to the bone size if that is what is needed to reinforce the bone to withstand the stresses. Two interesting conclusions I drew from several references are that first, what matters are cyclic stresses (as in walking) rather than static ones, and secondly the stresses encountered in 'ordinary life' are probably not significant. The corollary to the second is that very little study has been done on the response to much higher cyclic stresses over long periods, but what there is suggests it can be significant.
I note that bone remodelling does depend on (start with) collagen to a high degree. We have observed on many trips that after a few weeks walking our skin becomes more healthy and any wounds (cuts, scrapes etc) simply vanish in a day or two. This suggests that sustained walking beyond several weeks is boosting the collagen processes in our bodies, and this could influence bone remodelling.
Observation by many suggests that foot length grows a little bit but foot width grows a lot more. This would be consistent with the idea that bone remodelling is what is happening, since that seems to focus mainly on bone diameter rather than length.
As far as I could see, there has been almost no research on the physiological response to sustained long-distance walking by adults. Studies on babies and juveniles, on a few sedentary adults, or even on a few post-mortem bones: lots of that. In fact, some of the published articles did note this lack, but the authors did not seem inclined to pursue the matter.
Room for research!
Cheers
Physiology of Bone Formation, Remodeling, and Metabolism
Usha Kini and B. N. Nandeesh.
p 29:
Bone constantly undergoes modeling (reshaping) during life to help it adapt to changing biomechanical forces, as well as remodeling to remove old, microdamaged bone and replace it with new, mechanically stronger bone to help preserve bone strength.
p37:
Bones normally widen with aging in response to periosteal apposition of new
bone and endosteal resorption of old bone. Wolff’s law [see below] describes the
observation that long bones change shape to accommodate stresses placed on
them. Bone modeling is less frequent than remodeling in adults (Kobayashi
et al. 2003 ) .
p42:
2.4 Bone Remodeling
Bone remodeling is a lifelong process wherein old bone is removed from the
skeleton (a subprocess called bone resorption), and new bone is added (a
sub-process called ossification or bone formation). Remodeling involves
continuous removal of discrete packets of old bone, replacement of these
packets with newly synthesized proteinaceous matrix, and subsequent
mineralization of the matrix to form new bone
(Fernández-Tresguerres-Hernández-Gil et al. 2006 ; Fraher 1993 ). These
processes also control the reshaping or replacement of bone during growth
and following injuries like fractures but also microdamage (prevents
accumulation of bone microdamage through replacement of old bone with the
new one) (Turner 1998 ) which occurs during normal activity. Remodeling
responds also to functional demands of the mechanical loading. As a result,
bone is added where needed and removed where it is not required. This
process is essential in the maintenance of bone strength and mineral
homeostasis. The skeleton is a metabolically active organ that undergoes
continuous remodeling throughout life.
p 43:
The bone remodeling cycle involves a complex series of sequential steps
(coupling of bone formation and bone resorption). Bone balance is the
difference between the old bone resorbed and new bone formed. Periosteal
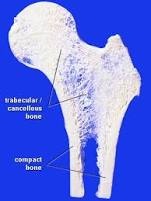
bone balance is mildly positive, whereas endosteal and trabecular bone
balances are mildly negative, leading to cortical and trabecular thinning
with aging. These relative changes occur with endosteal resorption
outstripping periosteal formation.
The main recognized functions of bone remodeling include preservation of
bone mechanical strength by replacing older, microdamaged bone with newer,
healthier bone and calcium and phosphate homeostasis. The relatively low
adult cortical bone turnover rate of 2–3 %/year is adequate to maintain
biomechanical strength of bone. The rate of trabecular bone turnover is
higher, more than required for maintenance of mechanical strength,
indicating that trabecular bone turnover is more important for mineral
metabolism.
p47:
2. Mechanical Factors
Remodeling is regulated by mechanical loading, allowing bone to adapt its
structure in response to the mechanical demands. Physical activity is
essential for the correct development of bone. It is believed that muscular
action transmits tension to the bone, which is detected by the osteocyte
network within the osseous fluid. On the other hand, the absence of
muscular activity, rest, or weightlessness has an adverse effect on bone,
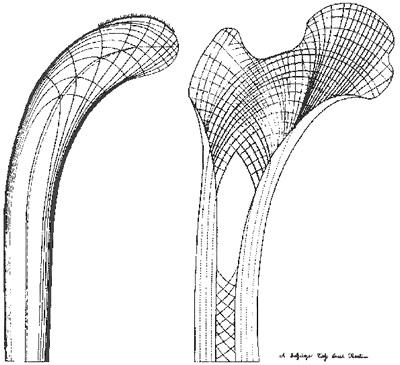
accelerating resorption. It is well-known that trabeculae tend to align
with maximum stresses in many bones. Mechanical stress improves bone
strength by influencing collagen alignment as new bone is being formed.
Cortical bone tissue located in regions subject to predominantly
tensile stresses has a higher percentage of collagen fibers aligned along
the bone long axis. In regions of predominant compressive stresses, fibers
are more likely to be aligned transverse to the long axis.
p52:
Collagen is the major structural protein of bone and comprises about 90 %
of the organic material. Collagen clearly contributes to the integrity
and strength of bone matrix, and defects in its production, for example, in
osteogenesis imperfecta, leads to bone of poor quality, susceptible to fracture.
Wikipedia
Wolff's law is a theory developed by the German anatomist and surgeon Julius Wolff (1836–1902) in the 19th century that states that bone in a healthy person or animal will adapt to the loads under which it is placed.[1] If loading on a particular bone increases, the bone will remodel itself over time to become stronger to resist that sort of loading.[2] The internal architecture of the trabeculae undergoes adaptive changes, followed by secondary changes to the external cortical portion of the bone,[3] perhaps becoming thicker as a result. The inverse is true as well: if the loading on a bone decreases, the bone will become weaker due to turnover, it is less metabolically costly to maintain and there is no stimulus for continued remodeling that is required to maintain bone mass.[4]
Mechanotransduction
The remodeling of bone in response to loading is achieved via mechanotransduction, a process through which forces or other mechanical signals are converted to biochemical signals in cellular signaling.[5] Mechanotransduction leading to bone remodeling involve the steps of mechanocoupling, biochemical coupling, signal transmission, and cell response.[6] The specific effects on bone structure depends on the duration, magnitude and rate of loading, and it has been found that only cyclic loading can induce bone formation.[6] When loaded, fluid flows away from areas of high compressive loading in the bone matrix.[7] Osteocytes are the most abundant cells in bone and are also the most sensitive to such fluid flow caused by mechanical loading.[5] Upon sensing a load, osteocytes regulate bone remodeling by signaling to other cells with signaling molecules or direct contact.[8] Additionally, osteoprogenitor cells, which may differentiate into osteoblasts or osteoclasts, are also mechanosensors and may differentiate one way or another depending on the loading condition.[8]
[My bolding]
Pub Med
http://www.ncbi.nlm.nih.gov/pubmed/8060014
Wolff's Law and bone's structural adaptations to mechanical usage: an overview for clinicians.
Frost HM.
Basic Multicellular Unit-based bone remodeling can lead to the removal or conservation of bone, but cannot add to it. Decreased mechanical usage (MU) and acute disuse result in loss of bone next to marrow; normal and hypervigorous MU result in bone conservation. Bone modeling by resorption and formation drifts can add bone and reshape the trabeculae and cortex to strengthen them but collectively they do not remove bone. >b>Hypervigorous MU turns this modeling on, and its architectural effects then lower typical peak bone strains caused by future loads of the same kind to a threshold range. Decreased and normal MU leave this modeling off. Where typical peak bone strains stay below a 50 microstrain region (the MESr) the largest disuse effects on remodeling occur. Larger strains depress it and make it conserve existing bone. Strains above a 1500 microstrain region (the MESm) tend to turn lamellar bone modeling drifts on. By adding to, reshaping and strengthening bone, those drifts reduce future strains under the same mechanical loads towards that strain region. Strains above a 3000 microstrain region (the MESp) can turn woven bone drifts on to suppress local lamellar drifts but can strengthen bone faster than lamellar drifts can. Such strains also increase bone microdamage and the remodeling that normally repairs it. Those values compare to bone's fracture strain of about 25,000 microstrain.